
Revenue Reclamation & Denial Mitigation
Advanced A/R Recovery & Aged Claim Liquidation
What sets Vexta RCM apart is our programmatic approach to legacy debt mitigation. When auditing your aged accounts receivable, we systematically dissect your 60, 90, and 120+ day tranches using advanced predictive analytics to prioritize high-value balances near timely-filing thresholds. Our team conducts detailed ledger reconciliations, cross-referencing initial clearinghouse 277 acknowledgments against current payer remittance data to trace unpaid claims. By deploying specialized recovery billers to aggressively confront historical underpayments and outstanding insurance balances, we rapidly compress your Days Sales Outstanding (DSO), injecting vital liquidity back into your medical practice.
Root-Cause Denial Management & Appeals
Vexta RCM replaces passive re-submissions with a rigorous, forensic denial management infrastructure. We ingest and analyze automated 835 Electronic Remittance Advices (ERAs) to map incoming Claim Adjustment Reason Codes (CARCs) and Remittance Advice Remark Codes (RARCs) straight to their upstream clinical or administrative points of failure. Whether resolving complex National Correct Coding Initiative (NCCI) edit conflicts, missing modifier 59 validations, or retroactive prior authorization disputes, our certified coders engineer robust, evidence-backed appeal packages complete with clinical documentation. We permanently patch your front-end workflows to ensure a sustainable 98%+ first-pass clean claim rate.
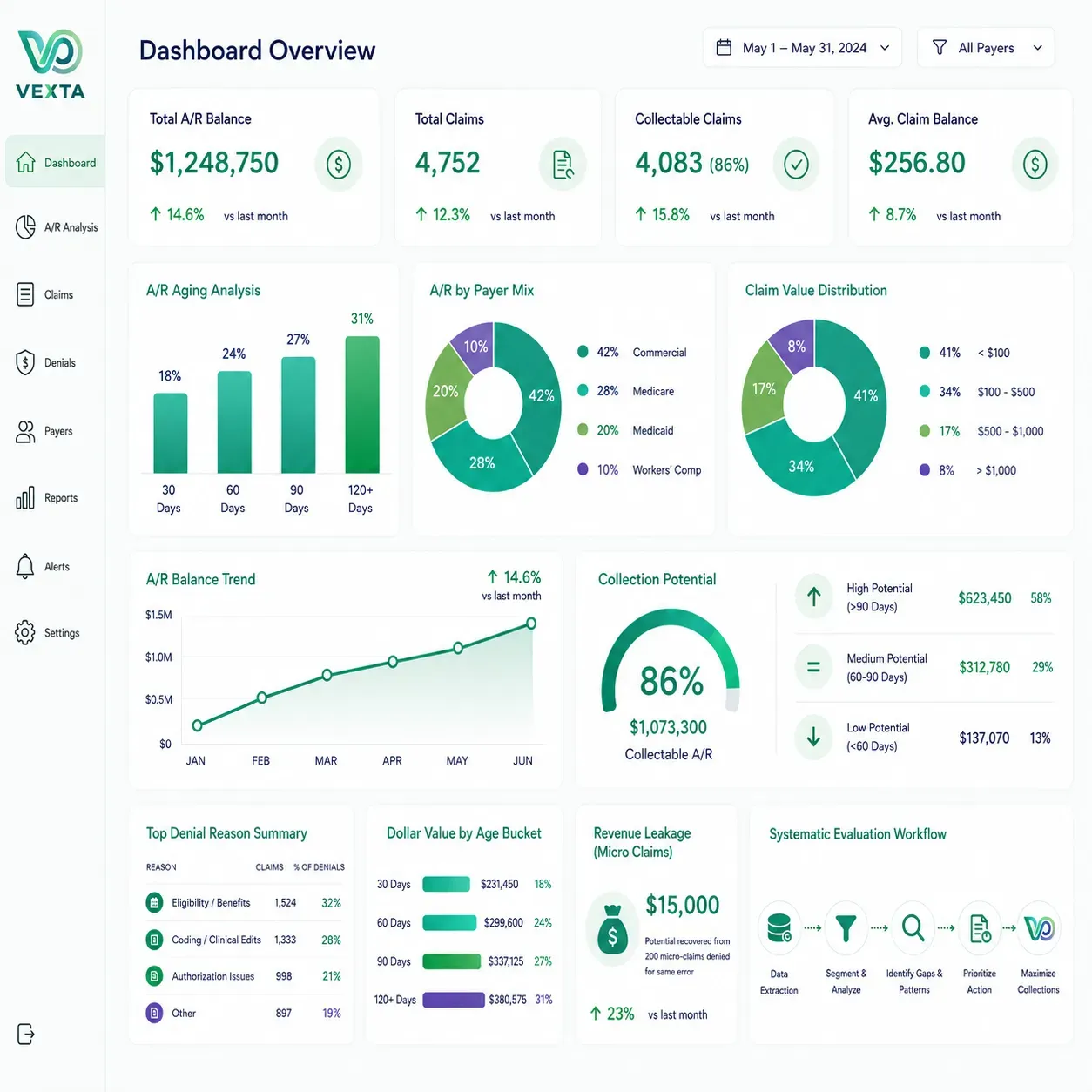
First pass clean claims rate
Reduction in A/R
Collection rate
The Vexta 4-Part A/R Recovery Framework
Backed by over seven years of specialized RCM leadership, our streamlined A/R recovery framework eliminates slow, legacy methods. We combine deep industry expertise with an agile, high-velocity workflow engineered to liquidate aging accounts rapidly and restore immediate cash flow to your practice.
1. Systematic Evaluation
As an A/R Recovery and Denial Management expert, I can tell you that the biggest mistake most practices make is treating their accounts receivable as a single, uniform bucket of money. It isn’t. True recovery requires a forensic, algorithmic approach to your data.
When we launch a data-driven audit of your entire aging matrix, we are doing much more than just looking at a balance sheet. We segment your A/R by specific parameters: age tranches (30, 60, 90, 120+ days), payer categories (Medicare, Medicaid, Commercial, Workers’ Comp), and dollar value.
While legacy billers only skim the “low-hanging fruit” by chasing high-dollar balances to make their monthly numbers look good, Vexta reviews every single collectable claim—regardless of size. Here is why this is a critical technical distinction:
- Preventing Timely-Filing Forfeiture
- The Aggregate Revenue Leak
- Isolating Cross-Payer Patterns
Every insurance payer has a strict window (often 90 to 180 days from the date of service) after which a claim becomes legally uncollectible. Legacy billers who ignore smaller claims allow hundreds of micro-claims to quietly expire behind the scenes.
A $75 denial might seem insignificant on its own, but when multiplied across hundreds of patient encounters, it represents a massive, systemic revenue leak. If a practice has 200 small claims denied for the exact same front-end registration error, that represents $15,000 in completely recoverable revenue that traditional billing companies write off as “uncollectible.”
By evaluating every single claim, we can cross-reference Clearinghouse 277 response logs and 835 Electronic Remittance Advices (ERAs). This allows us to catch systemic, low-dollar rejections that point to a bigger problem—such as an outdated fee schedule or a broken system configuration in your EHR.
We track down both major and minor outstanding balances, ensuring no earned dollar is left behind. We don’t just clear your dashboard; we mathematically maximize your net collection rate.
2. Strategic Prioritization
In accounts receivable management, time is your absolute enemy. Every day a claim sits unresolved, its probability of collection drops exponentially. As an expert in revenue cycle recovery, I look at an aging matrix not as a static list of debts, but as a ticking clock governed by strict legal contracts.
We meticulously analyze and segment your older unpaid claims based on tight filing deadlines, ensuring zero revenue expires before resolution. Here is the technical breakdown of how we execute this strategy to safeguard your cash flow:
Insurance companies place hard deadlines on when a corrected claim or appeal can be submitted. For instance, UnitedHealthcare typically requires appeals within 120 days of the initial adverse determination, while Blue Cross Blue Shield plans often mirror Medicare’s strict 365-day filing window. Our system automatically flags claims approaching these thresholds, elevating their priority status to prevent contractual write-offs.
Leveraging advanced analytical tools, our team outpaces strict payer requirements to aggressively capture your overdue payments. We cross-reference the TFL countdown with the expected allowed amount of the claim. This creates a “dynamic priority score.” A $5,000 surgical claim with 10 days left on its appeal window is instantly pushed to the top of an agent’s queue, followed immediately by high-volume, mid-dollar claims that aggregate to a substantial sum.
Insurers frequently use administrative friction—such as requesting medical records they already have or placing representatives on lengthy hold times—to run out the clock on your filing deadlines. We handle the relentless insurer follow-up around the clock, protecting your bottom line so you can focus entirely on patient care. Our team utilizes automated EDI (Electronic Data Interchange) tracking to bypass manual phone queues whenever possible, securing definitive payment commitments before the payer’s contractual liability expires.


3. Transparent Patient Communication
When a claim is processed and a portion of the balance shifts to the patient—whether due to high deductibles, co-insurance, or non-covered services—the RCM dynamic changes completely. As an expert, I know that patient balance collection is the most sensitive phase of the revenue cycle. Traditional collection agencies rely on aggressive, adversarial tactics that alienate patients and destroy the provider-patient relationship. At Vexta, we treat patient collections as a customer service and education workflow.
When outstanding balances shift to patient responsibility, we dispatch clear, easily digestible financial statements. Modern healthcare consumers are frustrated by confusing, jargon-heavy billing. We translate dense explanation of benefits (EOB) data into plain language, clearly showing what the insurance paid, what they adjusted, and the exact reason for the remaining patient balance.
Our technical approach to patient communication includes:
- Demystifying the Deductible
- Frictionless Omnichannel Payment Options
- Compassionate Propensity-to-Pay Workflows
Many patients do not fully understand their insurance plan architecture. Our trained billing representatives walk patients through their specific 835 remittance data, explaining how their annual deductible or out-of-pocket maximum directly correlates to the statement they received. This eliminates confusion and drastically reduces payment resistance.
To accelerate collections, our statements feature digital text-to-pay links, QR codes, and secure online patient portals. Providing immediate, secure payment channels directly targets the primary cause of unpaid patient bills: administrative inconvenience.
Instead of demanding immediate lump-sum payments that a patient may not be able to afford, we establish structured, automated payment plans within pre-approved practice parameters. This secures a predictable, recurring stream of patient revenue while ensuring patients feel supported rather than penalized.
4. Precision Correction & Resubmission
In the world of advanced RCM, a denial should never be treated as a permanent refusal of payment; it is simply a request for more precise data. Many legacy billing departments fall into the trap of “auto-reappealing”—meaning they resubmit the exact same claim multiple times hoping for a different result. This triggers immediate duplicate claim rejections and wastes valuable time.
Our dedicated task force systematically isolates every claim that is rejected, denied, or underpaid, ensuring no revenue is lost to administrative friction. When a denial hits our queue, our expert team dissects the specific 835 Electronic Remittance Advice (ERA) data, pulling the exact Claim Adjustment Reason Codes (CARCs) and Remittance Advice Remark Codes (RARCs) to identify the breakdown.
After executing precise clinical corrections and capturing missing data, we file targeted appeals to force rapid payer reconsideration. Our advanced correction protocol focuses on three critical technical layers:
We regularly encounter complex denials related to unbundling or missing modifiers (such as Modifier 25 or 59). Our certified coders audit the clinical documentation to ensure the services meet distinct procedural requirements, applying modifiers accurately to clear the payer’s automated edits.
If a claim is denied because a procedure code does not align with the patient’s diagnosis code according to payer-specific LCDs, we review the electronic health record (EHR). We map the precise ICD-10-CM codes that accurately reflect the clinical complexity of the encounter, ensuring full compliance.
We don’t just fix claims in isolation; we solve the root problem. We continuously monitor denial patterns, instantly updating our rules engine to eliminate recurring errors and permanently harden your revenue cycle against future rejections. If we notice a sudden spike in denials from a specific commercial payer regarding a pre-authorization format, we immediately adjust our front-end scrubbing rules. This updates the registration criteria for your front-desk staff, turning a reactive denial into a proactive, front-end block.
